




Carmela Augusta F. Dayrit-Castro, MD, FPDS
A “birthmark” is an irregularity on the skin which is visible at, or shortly after, birth. They are often benign and have no medical and psychological significance to the affected individual. However, there are some birthmarks for which medical attention should be sought. We name here a few of the more common types of birthmarks and mention when a child will need further evaluation by a physician.
BROWN BIRTHMARKS
Brown or pigmentary birthmarks are due to increased pigment or number of pigment producing cells in the skin.
Café au lait macules (CALMs) are common and are seen as a solitary or a few, flat, light brown or tan spots on the skin. CALMs are benign but they tend to be permanent. If there are multiple CALMs found on the skin, further evaluation is necessary to assess for hereditary conditions like neurofibromatosis.

Congenital melanocytic nevi are typical moles which appear as discrete bumps or elevations which range in color from light to dark brown to black and may have overlying thin hairs. These moles vary in size from small to giant. They tend to increase in size proportionately as children grow. Children with large or giant congenital melanocytic nevi need to be evaluated since they may have an increased risk to develop melanoma and to have pigment cells in the nervous system.

BLUE BIRTHMARKS
Dermal melanocytosis, commonly known as “Mongolian spots,” are blue-gray patches commonly located on the lower back and buttocks of infants. They appear more often in Asians and darker skinned individuals compared to lighter skinned individuals. These spots appear bluish because the pigment producing cells are halted on the lower layer of the skin, the dermis, en route to the upper layer, the epidermis. Mongolian spots tend to disappear by 3-5 years of age and rarely persist into adulthood. No further evaluation is needed for this. There are, however, pigment lasers that may be helpful for persistent dermal melanocytosis in adults.

RED BIRTHMARKS
Red birthmarks are due to the proliferation or growth of blood vessels on the skin.
A nevus simplex, or commonly called “salmon patch,” “angel’s kiss,” or “stork bite” is a pink to red mark usually found between the eyebrows, forehead, upper eyelids and nape of newborns. They tend to become more visible when a baby is crying or after physical exertion. These are formed because of the dilation of the smallest blood vessels or capillaries. They tend to disappear between 1 to 3 years of age but the ones located on the nape tend to persist. No further evaluation is usually required for this.

A port wine stain (PWS), is a more uniform, deeper red mark often located on the face. It can also appear elsewhere on the body, like on the arms and legs. A PWS appears because of an abnormal formation of capillaries on the skin, and may involve deeper tissues. Unlike a nevus simplex, PWSs tend to persist throughout life and may become thicker and develop red bumps on its surface during adolescence or adulthood. When a PWS appears on: (1) half of the face, (2) part of the face covering an upper or lower eyelid, (3) the midline of the forehead, or (4) a significant part of a limb, medical attention is recommended to assess involvement of the brain and eyes and discrepancy in limb size. There are also laser treatments available to help fade PWSs.

Infantile hemangiomas (IHs) often appear as soft, bright red bumps or elevations which are not, or barely, perceptible at birth. They are often mistaken as a mark from birth trauma. During the first 2 weeks of life, they begin to enlarge and may continue to enlarge until 3-5 months of age. Some IHs are deep and may appear as compressible skin colored or bluish green bumps that are recognized as infantile hemangiomas based on its growth pattern. Most IHs do not need treatment as they spontaneously resolve by 4-5 years of age. However, there are a subset of patients who need further evaluation and may require early treatment with oral medications during the first weeks of life. Early evaluation is needed when: (1) the IH is located on a “high-risk” location such as the eyelid, tip of nose, lip, midline chin and neck (beard area), ear, or groin as there is a risk for functional impairment, significant deformity, and ulceration; (2) there is a large IH on the face or on the lower back as this may be associated with other internal organ abnormalities; and (3) there are several infantile hemangiomas on the skin which could be a marker for having a liver hemangioma.

WHITE BIRTHMARKS
White birthmarks may appear due to decreased pigment or focal blood vessel constriction on the affected area.
Nevus depigmentosus is a whitish spot that is present since birth. They may be more difficult to see in lighter skinned individuals. There is decreased pigment or melanin in these spots. One spot is benign but if three or more are seen in a newborn, immediate evaluation for tuberous sclerosis complex should be sought.
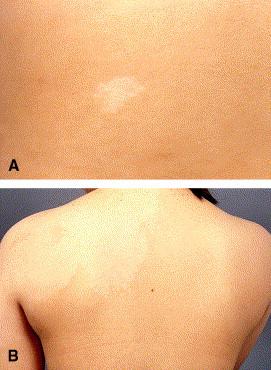
Nevus anemicus appears as a single or a group of whitish spots more often found on the trunk. They are asymptomatic and persist throughout life. It is an area of blood vessel constriction and when pressed at the border, can blend into the surrounding skin. As a solitary skin finding, no further evaluation is needed.

Other birthmarks
There may be less common and rare birthmarks which appear in various shapes, colors and textures—linear white or brown whorls and streaks; warty lesions; orange lesions on the scalp; tufts of hair; midline lesions. For more unusual birthmarks, your pediatrician may choose to refer you to a specialist for further evaluation and/or reassurance. But remember, when in doubt, it is always best to err on the side of caution and seek advice from your doctor.
REFERENCES:
Balin SJ. “Benign melanocytic neoplasms.” In: Bolognia JL, et al. Dermatology. (fourth edition). Mosby Elsevier, Spain, 2018:1954-88.
Baselga E. “Vascular malformations.” In: Bolognia JL, et al. Dermatology. (fourth edition). Mosby Elsevier, Spain, 2018:1805-27.
Chan YC. “Hypopigmentation disorders.” In: Eichenfield LF, et al. Neonatal and Infant Dermatology. (third edition). Mosby Elsevier, Spain, 2015: 369-87.
Hunt R “Neonatal dermatology.” In: Kang S, et al. Fitzpatrick’s Dermatology. (ninth edition). McGraw-Hill, USA, 2019: 1732-8.
Krowchuk DP, Frieden IJ, Mancini AJ, Darrow DH, Blei F, Greene AK, et al. Clinical Practice Guideline for the Management of Infantile Hemangiomas. Pediatrics. 2019 Jan;143(1):e20183475. doi: 10.1542/peds.2018-3475. PMID: 30584062.
Puttgen KB “Neonatal dermatology.” In: Cohen B. Pediatric Dermatology. (fourth edition). Elsevier, USA, 2013: 14-67.