Value at your desk. Contact Us
Value at your desk. Contact Us
Shereen Reine S. Rodriguez-Gimarino, MD, FPDS
Because food is at the heart of Filipino culture, dietary restriction comes up as a frequent question during consults with the doctor. Much of our cuisine is flavorful, comforting, and tend to be on the greasy side. No wonder that after a trip to the doctor, we’d be told to cut down on certain foods to improve our health. We come to realize the role food plays in diseases, oftentimes leading to assumptions.
“I have pimples because I’ve been eating a lot of [insert food item] lately,” is a statement us dermatologists have heard too often. You may have been advised some time ago that they have nothing to do with each other. This is because in truth, the role of diet as a trigger for acne took decades to establish. Even with new research coming out regularly, the verdict for certain foods is still not absolute. In the midst of the abundance of anecdotes out there, evidence-based research updates are continuous, so here we are, setting the record straight with the evidence to date:

Food that promote acne:
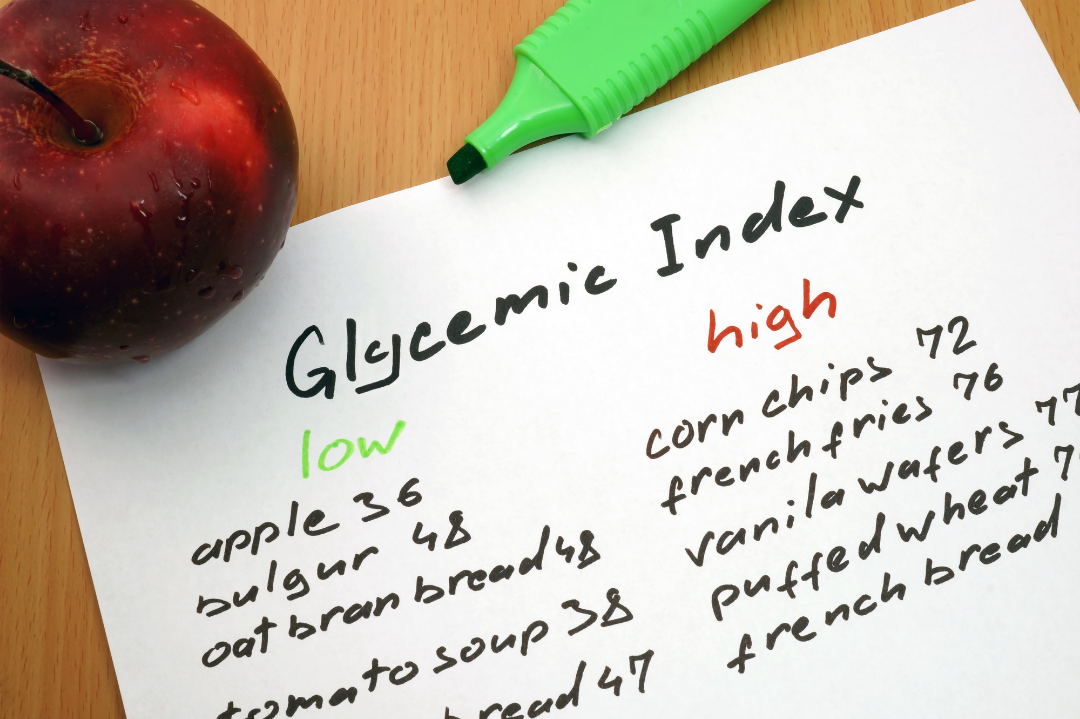
1) Sugary foods (High glycemic index / glycemic load foods)
Glycemic index is a numeric score that indicates how rapidly a certain food is digested and elevates your blood sugar. The more refined and processed the carbohydrate is, the faster it metabolizes into glucose (high glycemic index). On the other hand, glycemic load is a ranking system that takes into account both the glycemic index of a food and the portion that you consume.
Several studies support that diets high in glycemic index / glycemic load exacerbate existing acne, and can prolong its duration. Therefore, be wary of products that are refined and those that have “added sugar” on the label. Consume foods rich in fiber, fat and protein because these release glucose more slowly, so they have a lower glycemic index.
2) Dairy
Consumption of cow’s milk – whole, low-fat and skim, has consistently been linked to acne exacerbation and break-outs in several studies, including an advisory from the American Academy of Dermatology. Interestingly, dairy products such as yogurt and cheese were not observed to influence acne.

3) Whey protein supplements
Commonly drank as protein shakes for body building and fitness, whey is the main protein component (80%) of milk. Dermatologists often encounter severe acne in protein shake drinkers. Supported by studies, severe acne in these patients persists even with appropriate medication, and respond only when whey protein is discontinued.
Food that protect from acne:
1) Low glycemic index / glycemic load foods
Just as how high glycemic index / glycemic load foods aggravate acne, low glycemic index / load foods reduce the inflammation, count and severity of acne consistently across multiple studies to date.
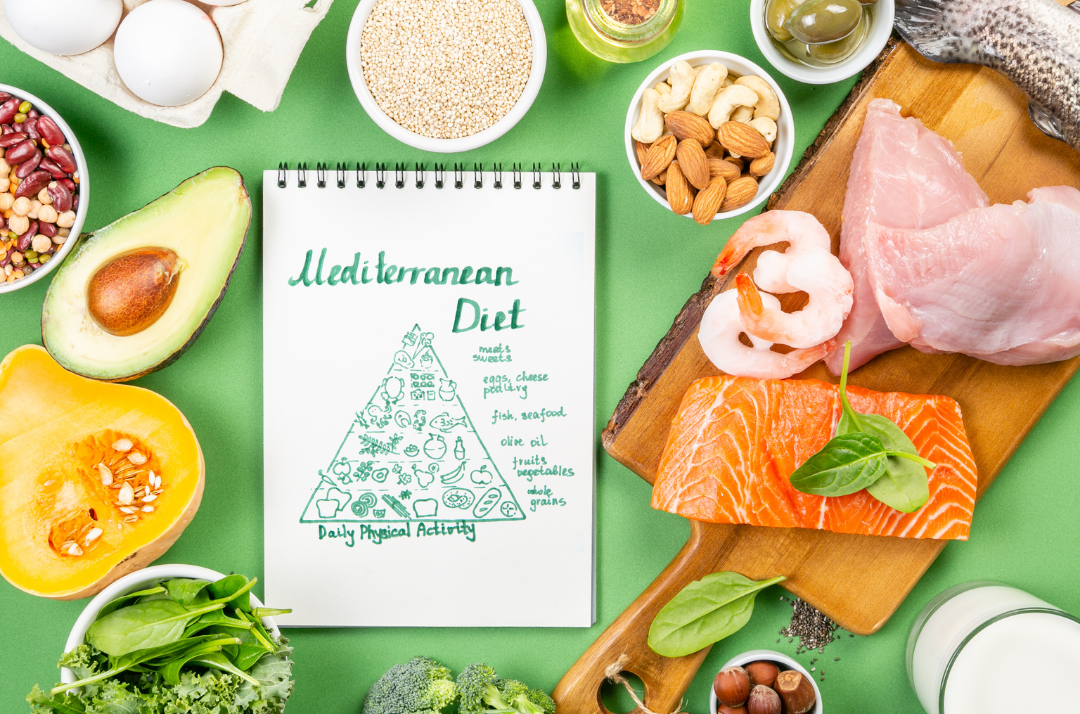
2) Omega-3 fatty acids and linoleic acid
These fatty acids, often associated with a Mediterranean diet and fish, have also been consistently observed to reduce inflammatory acne.
3) Vegetarian / vegan diet
Eating a fruit and vegetable-rich diet has been shown in recent studies to be acne protective.

Food that have been studied and deemed to not affect acne:
1) Salt
No association between salty food intake and acne was observed in studies.
2) Yogurt, cheese and other dairy products
As mentioned earlier, these milk products have no effect on acne in contrast to milk itself.
Food that have been studied but found to have insufficient evidence to either improve or aggravate acne:

1) Chocolate
This is food item is a popular question during an acne consult. Different studies varied in the brands and purity of chocolate (vs. its milk and sugar content) used, as well as the population involved, and have produced inconclusive results. Therefore, to date, chocolate is not yet proven to influence acne. Also be aware, however, that chocolates can easily become a high glycemic index food with dairy.
2) Probiotics
Probiotics have attracted attention for its gut health benefits over the recent years, and its effect on acne is not exempt from that. While initial studies are promising, further research and evaluation are needed to conclusively say it is beneficial for acne.
While there is some evidence supporting the relationship of acne and diet, this cannot replace proper evaluation of the cause of your acne and its corresponding management done in the setting of a Dermatology consult. Use the above information as a guide for your everyday food choices, rather than a treatment for your acne. Note that the evidence does not demonstrate that a certain type of food causes acne, rather they may influence existing acne positively or negatively.
Every year more and more evidences are unearthed about this topic, so stay tuned.

References:
by: Patricia Pontejos-Canivel, MD, DPDS

Acne is a hormonal skin condition that manifests as comedones known as “blackheads” or “whiteheads”. Comedones can become inflamed due to bacteria and turn into painful red bumps that become pustules or cysts. Our skin naturally produces oil or sebum and excess production can lead to clogging of the pores, this is what causes acne. Some factors that can contribute to the development or flaring of acne are:
When acne is left untreated, it can become severely inflamed and this can lead to scarring. Common types of acne scars are:

The best way to avoid scarring is to treat acne early and avoid picking on your skin. Different treatments can improve acne and acne scarring and this is best determined through a consultation with a board- certified Dermatologist. She/ he may suggest different treatments depending on the type of acne or acne scar you have.
“Maskne” or “Mask acne” is a new term that was coined due to the recent pandemic. It covers a wide range of skin conditions brought about by mask- wearing. Some cases may be real acne, but other conditions can also cause bumps on the skin. Some of these conditions are:
“Maskne” can be treated with proper diagnosis and treatment by a board- certified Dermatologist and should never be a reason to stop wearing masks in public. Some ways to prevent developing these conditions are:

Make sure to consult with a Board-Certified PDS Dermatologist!
REFERENCES:
Fitzpatrick’s Dermatology 9th edition
https://www.aad.org/public/diseases/acne/causes/acne-causes
by Katrina Canlas-Estrella, MD, FPDS
An allergic reaction is when a person’s immune system overreacts to an otherwise harmless substance (ex. Dust mite and peanut). In an allergic person, these substances are referred to as allergens. When a person is exposed to an allergen, his body produces antibodies that trigger the release of chemicals in the body like histamine, that causes the symptoms of allergies.
Allergic reactions vary, depending on several factors such as the allergen, the area of the body it affects, and the response of the person’s immune system. Symptoms can range from mild to severe. For example, food allergens can cause localized itching of the mouth, but they may also cause dangerous swelling of the tongue and the throat. Inhaled allergens like dust and pollen may cause itching of the eyes, sneezing, and wheezing. Some persons may be allergic to medications what can manifest as itchy rashes, hives, flushing of the skin, appearance of blisters, and swelling of the eyelids and the lips. Difficulty of breathing can occur in severe allergic reactions and can cause a potentially fatal condition called anaphylaxis.

Allergy can affect anyone. Some people are more prone to allergic problems when it runs in their family, while others may have no family history at all. People with other medical conditions such as asthma, eczema, chronic lung infections, and those with diseases that require intake of multiple drugs are more prone to developing allergies. Anything can be an allergen, Things that people are commonly allergic to include food (peanut, egg, soy, and shellfish), dust mite, tree and grass pollens, insect venom, medications, animal dander, and chemicals (hair dye, detergents).
Doctors can diagnose your allergies based on your symptoms. Your doctor may also perform tests (skin prick test, blood allergy test, and patch test) to find out what you are allergic to and how severe your allergies are.
Treatment depends on what your allergens are and how severe your reactions are to them. In general, you can avoid having allergic reactions by avoiding the allergens that cause them. Your doctor may recommend having an “allergy diary” and medications to relieve your symptoms. Allergists may recommend shots to certain allergens like dust and pollen.
A person with allergies should make a list indicating what he or she is allergic to and the type of allergy that he or she has. It is also helpful to inform their families, caregivers, schools, employees, and friends of what they are allergic to. Your doctor may also provide you with medications that you should carry with you at all times in case of an emergency. Early recognition of an impending allergic reaction will also prevent fatal complications.
by Michelle-Adeline Y. Noche-Apacible, FPDS
Atopic Dermatitis is commonly known to many as “eczema”, “asthma of the skin” or “hika sa balat.” Atopic dermatitis comes from the root word atopy or allergy. These can manifest as follows:
Infants from 0-24 months old: around the cheeks and outside parts of extremities. Just imagine the skin parts used when a baby crawls.
For 24 months old and above these manifest in flexural areas such as the skin on the inside of the elbows and knees.
Atopic Dermatitis is diagnosed through the use of criterias. Major criteria includes family history of allergy and recurrent skin condition. Minor criteria includes dry skin, keratosis pilaris (chicken skin), Dennie morgan folds (creases along the lower eyelids) etc.
The condition which involves increased IgE is usually inherited. This can present as allergic rhinitis (frequent sneezing in the morning), asthma or the same skin condition within the immediate or extended family members.
Patients often have dry skin since atopics lack the capability to retain moisture. Dryness causes pruritus (itch) can lead to severe scratching which damages the skin leading to infections. Atopics are also more prone to viral and fungal infections because their skin barrier is compromised.
Treatment starts with seeking a board-certified dermatologist from the Philippine Dermatological Society. Your Dermatologist will help you with finding the right moisturizer, maintaining a proper skin regimen, and avoiding bad habits.
Shorter baths periods with the proper moisturizer traps and retains the moisture preventing the escape of water from the skin. This prevents TEWL or Transepidermal Water Loss. Other further treatments may include proper use of topical corticosteroids, intake of antihistamines and prevention of secondary bacterial infections.
Although the journey in controlling your Atopic dermatitis may be frustrating, controlling and achieving a better daily life is definitely achievable. Most atopics are better by 17 years old. They then tend to get dry skin again when they approach their 40’s. An added fact: Did you know that most atopics have a high IQ?
So seek for a board-certified dermatologist now from the Philippine Dermatological Society and your journey to a better skin and quality life is on its way.
Sources (APA format):
American Academy of Dermatology Association. (n.d.). Eczema types: Atopic dermatitis diagnosis and treatment. Retrieved April 5, 2021, from https://www.aad.org/public/diseases/eczema/types/atopic-dermatitis/atopic-dermatitis-treatment
Md, A. P. S., & Md, A. M. J. (2015). Hurwitz Clinical Pediatric Dermatology: A Textbook of Skin Disorders of Childhood and Adolescence (5th ed.). Elsevier.
Allergic tendencies are associated with larger gray matter volumes
2018H Takeuchi, Y Taki, R Nouchi, R Yokoyama, Y Kotozaki, S Nakagawa, A Sekiguchi, K Iizuka, Y Yamamoto, S Hanawa, T Araki, CM Miyauchi, K Sakaki, T Nozawa, S Ikeda, S Yokota, M Daniele, Y Sassa, R Kawashima10.1038/s41598-018-21985-8Scientific Reports

Carmela Augusta F. Dayrit-Castro, MD, FPDS
A “birthmark” is an irregularity on the skin which is visible at, or shortly after, birth. They are often benign and have no medical and psychological significance to the affected individual. However, there are some birthmarks for which medical attention should be sought. We name here a few of the more common types of birthmarks and mention when a child will need further evaluation by a physician.
BROWN BIRTHMARKS
Brown or pigmentary birthmarks are due to increased pigment or number of pigment producing cells in the skin.
Café au lait macules (CALMs) are common and are seen as a solitary or a few, flat, light brown or tan spots on the skin. CALMs are benign but they tend to be permanent. If there are multiple CALMs found on the skin, further evaluation is necessary to assess for hereditary conditions like neurofibromatosis.

Congenital melanocytic nevi are typical moles which appear as discrete bumps or elevations which range in color from light to dark brown to black and may have overlying thin hairs. These moles vary in size from small to giant. They tend to increase in size proportionately as children grow. Children with large or giant congenital melanocytic nevi need to be evaluated since they may have an increased risk to develop melanoma and to have pigment cells in the nervous system.

BLUE BIRTHMARKS
Dermal melanocytosis, commonly known as “Mongolian spots,” are blue-gray patches commonly located on the lower back and buttocks of infants. They appear more often in Asians and darker skinned individuals compared to lighter skinned individuals. These spots appear bluish because the pigment producing cells are halted on the lower layer of the skin, the dermis, en route to the upper layer, the epidermis. Mongolian spots tend to disappear by 3-5 years of age and rarely persist into adulthood. No further evaluation is needed for this. There are, however, pigment lasers that may be helpful for persistent dermal melanocytosis in adults.

RED BIRTHMARKS
Red birthmarks are due to the proliferation or growth of blood vessels on the skin.
A nevus simplex, or commonly called “salmon patch,” “angel’s kiss,” or “stork bite” is a pink to red mark usually found between the eyebrows, forehead, upper eyelids and nape of newborns. They tend to become more visible when a baby is crying or after physical exertion. These are formed because of the dilation of the smallest blood vessels or capillaries. They tend to disappear between 1 to 3 years of age but the ones located on the nape tend to persist. No further evaluation is usually required for this.

A port wine stain (PWS), is a more uniform, deeper red mark often located on the face. It can also appear elsewhere on the body, like on the arms and legs. A PWS appears because of an abnormal formation of capillaries on the skin, and may involve deeper tissues. Unlike a nevus simplex, PWSs tend to persist throughout life and may become thicker and develop red bumps on its surface during adolescence or adulthood. When a PWS appears on: (1) half of the face, (2) part of the face covering an upper or lower eyelid, (3) the midline of the forehead, or (4) a significant part of a limb, medical attention is recommended to assess involvement of the brain and eyes and discrepancy in limb size. There are also laser treatments available to help fade PWSs.

Infantile hemangiomas (IHs) often appear as soft, bright red bumps or elevations which are not, or barely, perceptible at birth. They are often mistaken as a mark from birth trauma. During the first 2 weeks of life, they begin to enlarge and may continue to enlarge until 3-5 months of age. Some IHs are deep and may appear as compressible skin colored or bluish green bumps that are recognized as infantile hemangiomas based on its growth pattern. Most IHs do not need treatment as they spontaneously resolve by 4-5 years of age. However, there are a subset of patients who need further evaluation and may require early treatment with oral medications during the first weeks of life. Early evaluation is needed when: (1) the IH is located on a “high-risk” location such as the eyelid, tip of nose, lip, midline chin and neck (beard area), ear, or groin as there is a risk for functional impairment, significant deformity, and ulceration; (2) there is a large IH on the face or on the lower back as this may be associated with other internal organ abnormalities; and (3) there are several infantile hemangiomas on the skin which could be a marker for having a liver hemangioma.

WHITE BIRTHMARKS
White birthmarks may appear due to decreased pigment or focal blood vessel constriction on the affected area.
Nevus depigmentosus is a whitish spot that is present since birth. They may be more difficult to see in lighter skinned individuals. There is decreased pigment or melanin in these spots. One spot is benign but if three or more are seen in a newborn, immediate evaluation for tuberous sclerosis complex should be sought.
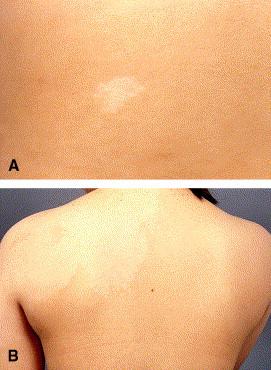
Nevus anemicus appears as a single or a group of whitish spots more often found on the trunk. They are asymptomatic and persist throughout life. It is an area of blood vessel constriction and when pressed at the border, can blend into the surrounding skin. As a solitary skin finding, no further evaluation is needed.

Other birthmarks
There may be less common and rare birthmarks which appear in various shapes, colors and textures—linear white or brown whorls and streaks; warty lesions; orange lesions on the scalp; tufts of hair; midline lesions. For more unusual birthmarks, your pediatrician may choose to refer you to a specialist for further evaluation and/or reassurance. But remember, when in doubt, it is always best to err on the side of caution and seek advice from your doctor.
REFERENCES:
Balin SJ. “Benign melanocytic neoplasms.” In: Bolognia JL, et al. Dermatology. (fourth edition). Mosby Elsevier, Spain, 2018:1954-88.
Baselga E. “Vascular malformations.” In: Bolognia JL, et al. Dermatology. (fourth edition). Mosby Elsevier, Spain, 2018:1805-27.
Chan YC. “Hypopigmentation disorders.” In: Eichenfield LF, et al. Neonatal and Infant Dermatology. (third edition). Mosby Elsevier, Spain, 2015: 369-87.
Hunt R “Neonatal dermatology.” In: Kang S, et al. Fitzpatrick’s Dermatology. (ninth edition). McGraw-Hill, USA, 2019: 1732-8.
Krowchuk DP, Frieden IJ, Mancini AJ, Darrow DH, Blei F, Greene AK, et al. Clinical Practice Guideline for the Management of Infantile Hemangiomas. Pediatrics. 2019 Jan;143(1):e20183475. doi: 10.1542/peds.2018-3475. PMID: 30584062.
Puttgen KB “Neonatal dermatology.” In: Cohen B. Pediatric Dermatology. (fourth edition). Elsevier, USA, 2013: 14-67.
by: Patricia Pontejos-Canivel, MD, DPDS
Boils are caused by a bacterial infection of the hair follicle. It presents as a painful red nodule on the skin that can start draining pus. This condition usually develops in areas that are prone to perspiration, friction and occlusion:
There are some factors that can predispose a person to developing boils such as:
Some boils may resolve on its own but if you are experiencing the following, consult a board- Dermatologist immediately:
Here are some tips to manage a boil at home:

References:
AAD website: https://www.aad.org/public/everyday-care/injured-skin/treat-boils-styes
Fitzpatrick’s Dermatology 9th edition
By Lonabel A. Encarnacion MD,FPDS, Elaine Marie Gutierrez-Villaroman MD,FPDS, Rizia Margate MD, Melissa See MD
Contact Dermatitis is skin inflammation or eczema that is triggered by substances that come in contact with the skin. These substances may be a chemical, biologic or a physical agent. Contact Dermatitis after a single or multiple exposure may be irritant or allergic. Let’s start with the more common irritant contact dermatitis (ICD) and later understand the more complex allergic contact dermatitis (ACD)
IRRITANT CONTACT DERMATITIS (ICD)
What is Irritant Contact Dermatitis?
Irritant contact dermatitis or ICD is a nonspecific, nonallergic response of the skin to direct chemical damage. That means it’s a random, automatic skin response to a threat. ICD is a localized skin reaction to an irritant. Irritant chemicals are soaps, detergents, acids and alkalis, industrial solvents, even rough clothing, etc. It is the most common occupational skin disorder and hands are most often affected.
How do we get Irritant Contact Dermatitis?
ICD may be acquired from exposure to an irritant substance. This irritant is a corrosive agent that triggers release of inflammatory chemicals mainly from the upper layers of the skin. It is an immediate skin defense reaction.
Who can get affected with Irritant Contact Dermatitis?
Any individual who comes in contact with an irritant for a sufficient amount of time and adequate concentration will most likely have ICD.
For instance, an employed dishwasher whose occupation exposes him to constant soap & water work setting is prone to ICD. All of us now in this pandemic, who constantly wash hands, disinfect with alcohol or use bleach sanitizers are prone to ICD.

What are the usual signs & symptoms of Irritant Contact Dermatitis?
Clinical manifestations of ICD are stinging, burning and itching with reddish bumps. There could be redness, mild swelling and scaling. There could also be thickening & cracking of the skin with constant exposure with the irritant chemical.
How is Irritant Contact Dermatitis diagnosed?
Diagnosis of ICD is primarily clinical and rests on the exclusion of other cutaneous diseases especially allergic contact dermatitis. When a patch test is done and result is negative, that negative result is consistent with Irritant Contact Dermatitis. (Just read on!)
What is the treatment for Irritant Contact Dermatitis?
Protect the skin. Use Barrier creams. Use Personal Protective Equipment such as gloves.
If in contact with the corrosive chemical, right away wash-off with water. Topical/oral steroids are used. And on those itchy skin areas, massage with moisturizers instead of scratching. This calms that irritated & angry skin!
ALLERGIC CONTACT DERMATITIS (ACD)
What is Allergic Contact Dermatitis?
Allergic contact dermatitis or ACD is a “s-l-o-w” delayed type hypersensitivity reaction of the skin to an allergen. Contact allergens are like hair dye, metals, jewelry, rubber, topical medications, skin care products, plants, chemicals and many, many more. The skin may develop allergy to these environmental substances. It’s not immediate and it takes time.

How can we get Allergic Contact Dermatitis?
ACD may be acquired by contact to an allergen of a sensitized individual or someone who came in contact with the allergen days, weeks or even years prior to appearance of the lesions. This means a prior exposure to an allergen chemical initiates this skin sensitivity. It is not an immediate type of skin reaction.
Who can get affected with Allergic Contact Dermatitis?
Persons with persistent or relapsing dermatitis may have ACD. All ages can get affected with ACD but is usually uncommon in young children and seniors above 70 years old.
What are the usual signs & symptoms of Allergic Contact Dermatitis?
ACD is characterized by itchy reddish bumps and blisters sometimes oozing. Thickened itchy plaques indicate a longstanding condition. These lesions usually come and go.
How is Allergic Contact Dermatitis diagnosed?
Patch testing confirms ACD. This test involves the application of common allergens on the patient’s back to re-create and document skin reactivity. Remember, a positive patch test is able to identify the allergen which must definitely be avoided to resolve the disturbing, recurrent dermatitis.
What is the treatment of Allergic Contact Dermatitis?
Identify and remove the cause. This is the definitive management of this recurrent, disturbing skin condition known as Allergic Contact Dermatitis.
Topical and /or oral steroids are effective in controlling the signs and symptoms. And do consult a board-certified dermatologist for best advice to avoid the allergens!
References:
Medscape https://emedicine.medscape.com/article/1049216 updated Aug 20,2020. Allergic Contact Dermatitis Updated Aug 20, 2020 Author Thomas N Helm, MD
Medscape https://emedicine.medscape.com/article/1049353-overview
Irritant Contact Dermatitis Updated: Nov 20, 2020 Author: Savina Aneja, MD
Wolff K, Johnson RA, Saavedra A, Roh E. Fitzpatrick’s Color Atlas and Synopsis of Clinical Dermatology. 8th ed. New York: McGraw-Hill Medical. 2017: 20-33Kang S, Amagai M, et al. Fitzpatrick’s Dermatology. 9th ed. McGraw-Hill Education. 2019: 395-427
Pia Victoria Velasco, MD, FPDS
A. FACE MASK SKIN CARE – Masks play an important role in preventing the spread of Coronavirus. However, regular use of masks can cause skin problems such as acne, rashes and even itchiness. To prevent these skin problems, her are some helpful skin care tips:
Heavy make-up is more likely to clog your pores and lead to break outs. If you cannot skip your make-up, look for products labeled as “non-comedogenic” which will not clog your pores. Use make-up on the areas on the eye area only and skip it on the areas covered by the mask to lessen the risk of maskne.

B. HOW TO COPE WITH HAND DERMATITIS- Hand washing has been a mainstay in controlling the spread of Covid-19. Unfortunately, frequent hand washing and use of alcohol have often left hands feeling dry and irritated. Here are some helpful tips on how to keep Coronavirus away without compromising care for our hands:

References:
1. cdc.gov
2. pds.org: Recommendations for Addressing PPE-related Skin Care Issues during the COVID-19 Crisis
3. AAD COVID-19 Coronavirus Resource Center
Heirich Fevrier P. Manalili, RPh MD DPDS
Martha Joy Bruan-Tapales, RPh MD FPDS

There had been a lot of people (including doctors) who interchange a cream and an ointment. Knowing the difference between the two can help the patient and clinician decide on which preparation would benefit their condition more.
Ointments are semisolid preparations that contains lipid or hydrophobic ingredients intended for external application to the skin or other mucosal membranes1,2. It usually contains less than 20% of water and other volatile ingredients (eg. Ethanol), and more than 50% hydrocarbons and waxes1,2. They are designed to soften or melt at body temperature, spread easily, and have a smooth, non-gritty feel and appear translucent1. They are typically used as emollients to make skin pliable, barriers to prevent noxious substances from coming in contact to skin and vehicles for hydrophobic drugs1,2.
Creams are semisolid dosage forms containing one or more drug substances dissolved or dispersed in a suitable emulsion base1,2,3. They are more considered to be more fluid to other dosage forms1. They are usually found to have whitish, creamy appearance, due to scattering of light from dispersed phases (eg. Oil globules)1. Creams can either be on a water-in-oil emulsion (eg cold cream) which can be used as a softening and cleaning agent for make-ups1,2. On the other hand, it can also be in an oil-in-water emulsion (eg. Vanishing cream) which when rubbed on the skin, the water evaporates, leading to increased concentration of a water-soluble drug in the oily film which can adhere directly to the skin1,2.
Implications in Dermatology practice
As a vehicle, ointments have higher penetrability and are useful for thickened skin over palms and soles and over lichenified skin (eg. ichthyoses, psoriasis)4. The downside is that they are relatively greasy and messy to use. On the other hand, creams are less greasy and are more suited for moist and weeping areas of the skin (eg. Wounds with pus, blood and serum)4. Creams are preferred over ointments for mucosal areas because they are easier to spread and remove2.
In using topical steroids, the vehicle play an important role in determining the potency of the active ingredient4. For example, Mometasone furoate 0.1% cream is classified under Mid-potent (Class IV) while its counterpart Mometasone furoate 0.1% ointment is classified as high-potent (Class II).
References:
By: Bernadette Caluya, MD, DPDS
What is Dandruff?
Dandruff is a common skin condition where dry scales flake from the scalp. It is not contagious but it can be itchy and embarrassing to those who have it. It can occur across all age groups.It can be chronic and recurrent for many years. Dandruff may worsen during low temperature seasons and may also be associated with immunodeficiency and stress.
What are the symptoms?
It can be associated to the following symptoms:
-itchiness
-oily scalp
– scales on your scalp, eyebrows, back of ears, sides of the nose, chin, chest and upper back
What causes dandruff?
– seborrhea or increased sebum production in the scalp
– some cases are associated with increase of a fungus called Malassezia furfur on affected skin
– skin conditions like Seborrheic Dermatitis, Psoriasis, Eczema or Contact dermatitis to hair products
How to treat dandruff?
It is advisable to seek consult to a board-certified dermatologist before starting any treatment so that one’s condition will be assessed adequately and proper treatment will be prescribed.